
Cholera outbreaks are frequent and steadily increasing in India, shows recent surveillance data. However, this is only the tip of the iceberg and the disease continues to be grossly under recognised and underreported, informs this paper titled 'Cholera outbreaks in India, 2011–2020: A systematic review' published in the International Journal of Environmental Research and Public Health.
What is cholera
Cholera is an acute infection caused by intake of water or food contaminated with the bacterium Vibrio cholerae, which is extremely virulent and can cause severe acute watery diarrhoea. It takes between 12 hours and 5 days for a person to show symptoms of cholera after ingesting contaminated water or food.
Untreated water sources can carry the risk of cholera and cholera causing bacteria are often found to hitchhike on the surface of the bodies of copepods – small crustaceans found in freshwater.
Copepods play a central role in aquatic food web and can be found in high numbers in any aquatic habitat, including moist soils and subterranean environmen and serve as high energy food for fish and other organisms. Copepods are known to harbour a range of vectors such as cholera bacteria and others such as tapeworms, flukeworms etc that cause infectious diseases.
What causes cholera
The heavy reliance of communities on untreated water sources for daily water needs such as drinking, bathing, cooking, and washing utensils increases the risk of ingesting copepods, carriers for cholera-causing bacteria Vibrio cholerae. Copepod numbers can increase due to fluctuations in several climatic factors such as increased water temperature, thus increasing the possibility of ingesting an infective dose of Vibrio cholerae through copepod infested water.
Once infected, a person can spread cholera by contaminating drinking water sources or food due to unhygienic practices such as lack of handwashing following defecation. Lack of hygiene, poor nutritional status, lack of clean surroundings and poor socioeconomic conditions are enabling factors for the causation and spread of cholera.
Cholera is endemic in India and shows seasonal dynamics with a high number of people being affected during hot, humid and rainy seasons. The seasonality of cholera outbreaks is also influenced by environmental conditions and climate, host-immunity and health behaviour.
Drivers of cholera
While cholera is rampant in India, the drivers of these outbreaks have not yet been systematically analysed. The paper discusses the findings of the study that analyses the trends in cholera outbreaks in India over the last ten years and changes in the pattern of drivers of cholera.
The study found that:
- There were 565 outbreaks reported between 2011 and 2020 resulting in approximately 45,759 cholera cases and 263 deaths.
- These outbreaks occurred in 24 of the 36 states and union territories (SUTs) at least once between 2011 to 2020.
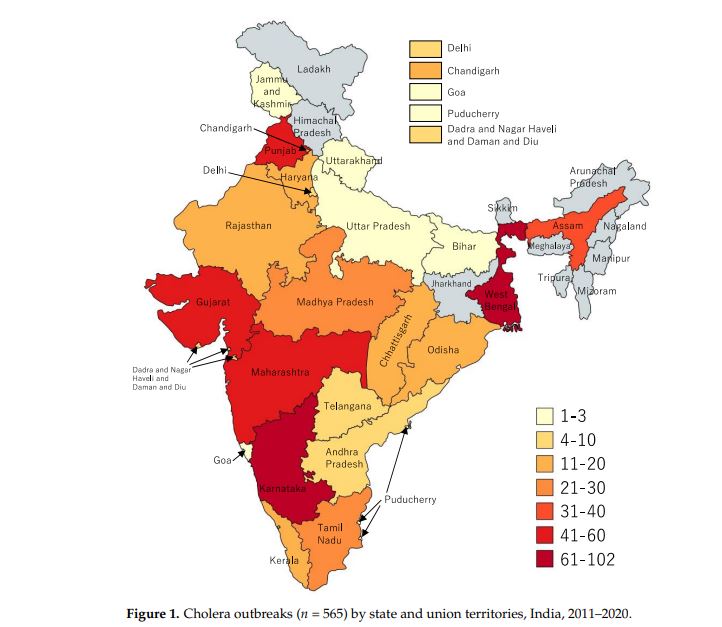
- The occurrence of outbreaks varied greatly across the years. The highest number of reported outbreaks was recorded in 2016 and lowest in the year 2020.
- Karnataka reported the most outbreaks followed by West Bengal, Maharashtra, Gujarat, Punjab, Assam, Madhya Pradesh, Tamil Nadu and Odisha.
- As high as 90 percent of the outbreaks affected people living in rural areas.
- Explosion of outbreaks occurred during the monsoon season in most of the SUTs and the peak was observed in July.
- Among the reported outbreaks, as high as 91 percent of the infections occurred due to consumption of contaminated drinking water or exposure to unimproved water sources and 9 percent due to lack of sanitation and hygiene.
- Transmission routes included leaking water pipelines, inadequate sanitation or hygiene, including open defecation and food borne transmission due to mixing of people in the house or during social gatherings.
- A decreasing trend was observed over the years in the number of outbreaks linked to leaking water pipelines.
- Cholera outbreaks were specifically found to be linked to the use of contaminated sources such as pond water, wells, piped water, handpumps, leaky water pipelines, consumption of untreated municipal water and unboiled water.
- Paddy cultivation during the rainy season was found to be linked to cholera outbreaks as farmers often practised open defecation and consume drinking water from open wells and rivers in the vicinity.
- Migration of people from rural areas to periurban slums and back was also found to be linked to the spread of cholera. For example, when there was no work on the farms, people from rural areas migrated to urban areas in search of work and then returned back to their farms during the rains.
- Many outbreaks happened due to faecal contamination of drinking water. Some outbreaks could be linked to natural disasters such as flooding or cyclones that led to water contamination due to overflowing toilets, canals, and drains, interrupted water distribution, or shortages of drinking water supply leading to the usage of unimproved water sources. Shortage of drinking water during the summer also forced people to use contaminated water
The Indian government has been making attempts to actively invest in water, sanitation and hygiene programmes over the years (e.g., Swachh Bharat Mission),. However, challenges remain such as coping with inhouse contamination of drinking water, inadequate water infrastructure that can lead to contamination of drinking water, and a shortage of water supply that can force people to use unimproved water sources.
These findings call for the need to emphasise handwashing behaviour with soap and water. However, households with limited access to handwashing resources (soap and running water) will not be able to wash their hands often. The need to develop and maintain hand-washing facilities alongside providing logistics to support hand-washing is thus urgent.
But only water availability is not enough on its own and can neither automatically translate into higher handwashing and effective health benefits as it will require behavioral changes that might be difficult to maintain over time, argues the paper. Thus, educational efforts along with social mobilisation, support for behavioral change and counselling will be greatly useful to reduce exposure to Vibrio cholerae.
"Strategies to prevent cholera should focus on targeted use of cholera vaccines, provision of safe drinking water, chlorination of water sources, regular disinfection of tube wells and wells, filtering water, supplying oral rehydration salts (ORS), antibiotics and bleaching powder, promotion of good personal hygiene and sanitation, education and awareness campaigns, safe food handling, proper sewage disposal, construction of drainage water away from the water pipelines, and long-term disease surveillance"( Muzembo B. A et al. (2022) Cholera outbreaks in India, 2011–2020: A systematic review. International Journal of Environmental Research and Public Health, 19 (5738), pp 15), argues the paper.