
Arsenic, a commonly found element in nature is often referred to as a toxic substance and ranks number one in the 2001 priority list of hazardous substances and disease registry defined by WHO.
Arsenic can naturally be found in rocks, especially in unconsolidated sediment aquifers that can lead to contamination of groundwater resources. Arsenic contamination of groundwater can also occur due to human induced anthropogenic activities such as copper mining.
The general population can be exposed to arsenic through contamination of drinking water and food. High concentrations of arsenic in water and food can as a major risk to human health as arsenic is known to be highly carcinogenic besides being teratogenic (can cause abnormalities in the foetus) and mutagenic (induce genetic mutations).
Extent of arsenic contamination of groundwater resources
Arsenic contamination of groundwater has been found to affect as high as 500 million people around the globe. The South and Southeast Asian Belt is the most arsenic polluted and includes countries such as India, Bangladesh, Nepal, Vietnam and China. While groundwater plays a vital role in meeting the rising domestic, industrial and irrigation needs in India, high arsenic in groundwater has been reported in shallow aquifers from ten states in the country.
Alluvial aquifers are the main source (90 percent) of arsenic in India while hard rock aquifers account for only 10 percent and include the states of Karnataka and Chattisgarh. In Karnataka, arsenic is reported in association with sulfide mineralisation, especially arsenopyrite, which is mainly restricted to the gold mineralised areas covering parts of Raichur and Yadgir districts. In Chattisgarh, it has been found to be associated with Kotri lineament. However, the deeper aquifers of India (>100 m) are free from arsenic.
Currently, twenty states that include West Bengal, Jharkhand, Bihar, Uttar Pradesh, Assam, Gujarat, Haryana, Madhya Pradesh, Punjab, Arunachal Pradesh, , Karnataka, Tamil Nadu, Himachal Pradesh, Telangana, Andhra Pradesh, Orrisa, Nagaland, Tripura, Manipur, Chhattisgarh) and 4 Union territories (Delhi, Daman and Diu, Puducherry, Jammu and Kashmir) are affected by arsenic contamination.
Arsenic contamination and reproductive health, the linkages
The World Health Organisation (WHO) guidelines have placed 10 parts per billion (ppb) on arsenic in drinking water as a safe limit.
While estimates suggest that up to 220 million people are exposed to arsenic contamination, with a majority of them residing in Asia, arsenic is not routinely included in water quality testing parameters making it difficult to understand the scale of the problem, informs this paper titled 'Is living in a region with high groundwater arsenic contamination associated with adverse reproductive health outcomes? An analysis using nationally representative data from India' published in the International Journal of Hygiene and Environmental Health.
India and Bangladesh have some of the highest levels of groundwater arsenic detected in drinking water. India’s National Drinking Water Program aims to provide safe water to rural households by 2024 through provision of piped water supply and introducing technological interventions for potable water. Thus, installation of community water purification plants have been recommended in arsenic-affected habitats for availability of safe water for drinking and cooking.
And high levels of arsenic in drinking water can be fatal for humans. Chronic arsenic exposure can affect multiple organs and cause skin problems, damage to peripheral blood vessels, diabetes, hypertension and skin, bladder, kidney, and lung cancers.
While arsenic is suspected to affect reproductive health (RH) outcomes among women, there are very few studies that have tried to explore the relationship between the two and the mechanisms that lead to arsenic-induced adverse RH outcomes among women.
The paper discusses the findings of a study that explores the association between adverse reproductive health outcomes among women and spatial district wise distribution of arsenic affected areas. Data from the female respondents collected from India’s nationally representative District Level Health Survey, Round 3 (DLHS=3) was compared with modelled, gridded groundwater arsenic dataset to 1 km spatial resolution to assess district-level associations between groundwater arsenic levels and still births, recurrent pregnancy loss (RPL) and infertility among women. A total of 643,944 women from the age group of 15–49 were included in the analysis.
The study findings:
The study found that the average district proportion of women experiencing at least one stillbirth was 4.3 percent (range 0.3–16.7%), while women experiencing RPL was 3.3 percent (range 0.0–12.1%), and any infertility was 8.1 percent (range 0.7–20.7%).
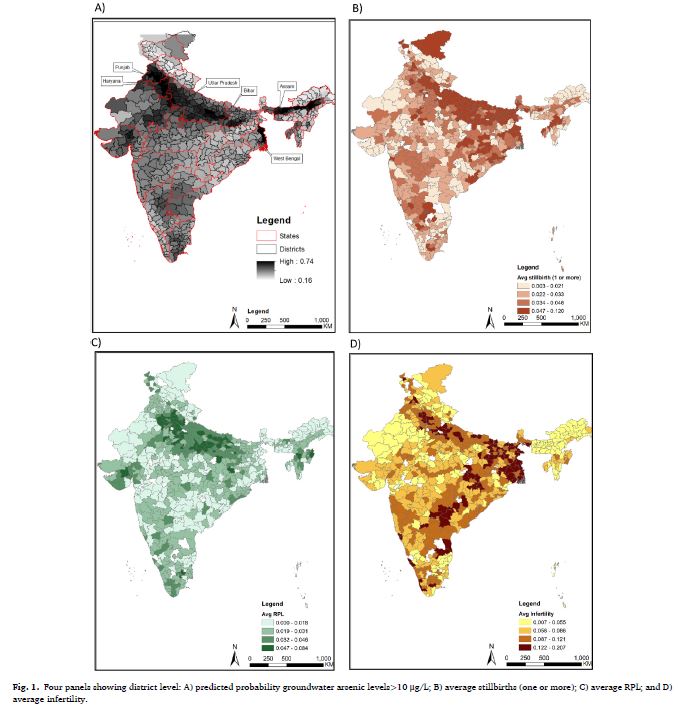
When spatial distribution of arsenic in the groundwater above the WHO 10 μg/L cutoff and the average district-level rate of stillbirth, RPL and infertility were mapped, it was found that the maps suggested a similar spatial pattern for both reproductive health outcomes and arsenic levels. Stillbirth and RPL showed highest district level rates in Bihar, Uttar Pradesh, and districts in Rajasthan. For infertility, rates were highest in West Bengal, Bihar, Uttar Pradesh and Chhattisgarh, along with southern states of Andhra Pradesh and Telangana.
The study found a strong relationship between arsenic contamination of groundwater and RPL and infertility. The study found a strong spatial association of adverse RH outcomes with the spatial distribution of arsenic at the district-level.
The study is one of the first national and district-level analyses of the association between high levels of groundwater arsenic contamination and adverse reproductive health and provides a possible explanation for the geographic variation in infertility concentrated along parts of the Gangetic basin, argues the paper.
The paper argues that this geographic variation in adverse reproductive health outcomes warrants deeper examination of a wider range of environmental determinants at both the state and district level. While regulation of infertility treatment practices is needed, there is an urgent need to focus on underlying determinants such as arsenic to prevent poor reproductive outcomes among women at the policy level besides furthering efforts to mitigate arsenic exposure in high risk areas and among vulnerable and underserved populations.
While climate change may exacerbate exposure and effects of environmental toxins in the future, studies such as these can be of great help in further exploring the associations between adverse health outcomes and environmental toxins in India and across the globe, argues the paper.
The paper can be accessed here